Hiring Tips: Right Staff and Patient Type Determination
March 11, 2022
Hiring staff who will fit your practice and stay longer than a minute can help save you money and time. In this installment, we share some hacks for interviewing and hiring that put the odds of hiring the right talent in your favor. We’ll also help dispel some myths to help you differentiate new from established patients, and provide a guide to make your coding more accurate.
Staffing issues are a struggle for many urgent care providers. And replacing team members costs your business time and money. Here are some stats to consider from career planning site Zippia.com when you’re trying to hire new team members.
Making sure your new hires are the right fit for your business helps you cut these costs and shorten the time it takes to get someone up and running. Use these four strategies to help secure your dream team.
Historically, organizations may have utilized one-on-one interviews with a quick couple of rounds involving only a couple of candidates. Involving more people in the process has several benefits that pay off.
Use phone screenings by a dedicated employee or HR company to eliminate unqualified candidates early in the process – especially when you have a lot of applicants. It saves time for everyone. This person should have specific “rule-out” questions and a list of soft skills you’re looking for depending on the position. Only pass prequalified people through to second interview.
Once you move candidates forward, you have a few options: a group interview, serial interviews, or even a meal interview. Each has benefits and drawbacks. Keep the open position in mind when determining the right strategy for you. A customer-facing position will have different requirements from a data entry position. Choose the interview style that best reflects the position.
With so many remote positions available, remote interviews are more common than ever and can involve multiple interviewers. If teamwork is important in the position, it might be a good opportunity to get multiple team members to prepare and ask questions of the candidate.
Before you begin the process, decide who needs to be involved – and look to the future of your organization. You know your immediate needs but think about how this role can evolve as your business grows and changes. What skills does a candidate have that may help them grow their own career within your organization? Keep that in mind when choosing who will be involved in your interview process and during each individual interview.
If you need to hire a lot of people quickly, or if you work for a big organization that has a very formal interview process, it may make sense to have a very structured interview planned, which allows you to evaluate multiple candidates by the exact same questions and standards. But if you have more flexibility, a less structured or unstructured interview may leave space to gauge rapport. You may have an easier time evaluating whether a person has that spark of passion that can help your organization grow in the best ways, or whether they’d be a good fit with your team and culture.
You have options within any kind of interview to evaluate a candidate’s mettle, too. Situational, behavioral, and performance-based interviews allow you to see how a person responds (or imagines they’d respond) in various scenarios. Some questions may allow a candidate to speak from actual experience and some allow them to imagine how they’d react. These interview approaches can tell you about a candidate because you can glean information from their actual answers, as well as body language or the tone of voice — and help you determine whether they would be a good fit in reality, not just on paper.
Bottom line: Approaching interviews with a lot of preparation helps everyone, in the short and long term, and can even save you money by allowing you to home in on the right candidate (and eliminate those that don’t fit) from the first round.
There’s more to determining patient status than the 3-year rule
With all the changes to the office/outpatient evaluation and management (E/M) services in the last few years, it’s easy to forget that some guidelines for 99202-99215 (Office or other outpatient visit for the evaluation and management of a new/ established patient …) have remained the same. CPT® guidelines for determining whether a patient is new or established to your practice are a good example of guidelines that haven’t changed.
But there are still some lingering myths about the guidelines that need to be dispelled. Here are three of the most common, along with two very good reasons why you need to determine patient status correctly.
Consider a patient who has not previously seen any of the physicians or qualified healthcare professionals (QHPs) in the practice and who comes in solely for a flu immunization. A nurse administers the shot, and you report 90471 (Immunization administration (includes percutaneous, intradermal, subcutaneous, or intramuscular injections); 1 vaccine (single or combination vaccine/toxoid)), along with the appropriate code for the flu vaccine product, but you report no office/ outpatient E/M service on that date of service. Several weeks later, the patient returns. Your provider performs an office/ outpatient E/M service at that time, and you report the service with an established patient code.
This coding would be incorrect. CPT® defines an established patient as “one who has received professional services from the physician/qualified health care professional or another physician/qualified health care professional of the exact same specialty and subspecialty who belongs to the same group practice, within the past three years” (emphasis added). CPT® also states, “Solely for the purposes of distinguishing between new and established patients, professional services are those face-to-face services rendered by physicians and other qualified health care professionals who may report evaluation and management services reported by a specific CPT® code(s)” (emphasis added).
In the scenario above, the returning patient has only received a flu shot from a nurse and received no professional services from the physician or other QHP in the practice. As such, the patient does not meet the CPT® definition of “established.”
So, in this case, you should use a new patient office/outpatient E/M for the first encounter with a provider after the flu shot and use an established office/outpatient E/M for the E/M services provided during the patient’s subsequent encounters.
This myth is particularly tricky to dispel, as often different providers practicing in different specialties may be billing under the same group taxpayer identification number (TIN), making it seem like the billing is the same regardless of provider specialty.
However, TINs are not the determining factor to determine specialty and subspecialty differences. Providers also have different taxonomy codes that indicate different specialties.
As an example, take an adolescent patient who has been seen by a pediatrician and who then transitions into adult care and is seen by a family physician in the same practice for the first time. The pediatrician and family physician both bill under the same practice TIN, but they have different taxonomy codes and are therefore regarded as practicing in a different specialty.
In this case, the patient’s first appointment with the family physician would be as a new patient, assuming the patient had not seen that provider or another family physician in the group practice within the three years prior to that first appointment.
Because 99211 (Office or other outpatient visit for the evaluation and management of an established patient that may not require the presence of a physician or other qualified health care professional) does not require the presence of a physician and requires no history, exam, or medical decision making (MDM), you may assume you can use the code for a new patient who receives office/outpatient E/M services from a nurse practitioner, (NP), a physician assistant (PA) or any other nonphysician practitioner (NPP). However, this is a myth for three very good reasons.
There are exceptions during the Public Health Emergency (PHE) so what follows is general guidance.
First, “CPT® describes the 99211 service as being for an established patient, so it cannot be used for a new patient,” Holle explains.
Second, the code can only be for established patients because if the service is provided by someone other than a physician or other QHP, the service will still be reported under the supervising physician or QHP’s provider number. Medicare regards this service as incident to the physician, and you cannot provide incident-to services to a new patient because one of the many requirements for incident-to reporting is that there must be a course of treatment in place, which isn’t true for a new patient.
Lastly, QHPs, including NPPs, are eligible to report any appropriate level of E/M service. Thus, if a QHP sees a new patient, that encounter may be reported with 99202 at a minimum, which is not only more appropriate coding but also pays better than established-patient code 99211.
Why Is the new/established patient distinction important?
Incorrectly identifying a new patient as established poses a billing risk. The reimbursement is higher for a new patient at the same level of service, due to the extra work typically involved in taking the patient’s history and diagnosing new conditions.
But the second reason your office needs to make the distinction correctly may be more important – compliance.
Whether your clinic stepped up to offer telehealth services during the pandemic or are just getting started, there’s no time like the present to assess your compliance measures and make improvements.
The public health emergency triggered rapid growth in telemedicine services and remote patient monitoring. Some clinics who had not been offering these services jumped on board to make sure they could continue to deliver patient care with less risk to patients and staff.
With the gradual return to normal visit volume levels, you have the opportunity to take a good look at your telemedicine operations and do an internal audit and answer these questions.
If you’re interested in expanding your telehealth services because your patients prefer the flexibility, you may want to consider how to make it better as you grow that sector of your business.
Telehealth is not likely to replace all face-to-face encounters because a clinician cannot always assess a condition and provide an accurate diagnosis without a face-to-face visit, but providers should still be prepared to offer the services and remain compliant while doing so.
Avoid these shortcuts or you may muddy the waters
With the nearly full adoption of electronic health records (EHRs) by the healthcare community, the stigma providers have long carried for their hard-to-read handwriting is losing steam. However, some medical shorthand is problematic regardless of readability. Pocket this chart, with information from The Joint Commission, to make sure you don’t run afoul of best practices.
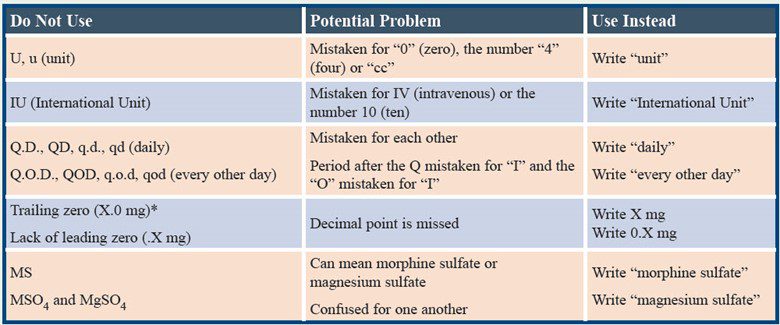
Note: “The prohibited list applies to all orders, preprinted forms, and medication-related documentation,” The Joint Commission says in a 2021 FAQ.
Maybe. Modern Healthcare has reported that only about $7 billion remains to reimburse providers that treated, tested, and vaccinated uninsured COVID-19 patients. While it is predicted that these funds will be refurbished, if you are behind on obtaining your temporary ids, it is a good idea to catch up. Experity will continue to monitor this situation.
As of 01/24/2022, two monoclonal antibody treatments are no longer authorized for use in the United States.
This change was made by the FDA because data show these treatments are “highly unlikely to be active against the omicron variant”.
There are other treatments available.
Interested in more urgent care tips, best practices, and industry updates? Check out our January and February installments.
Interested in more? Our RCM experts use smart solutions and best practices to stay on top of revenue cycles and reimbursement.
Join over 20,000 healthcare professionals who receive our monthly newsletter.

Join over 20,000 healthcare professionals who receive our monthly newsletter.