How to Improve E/M Coding Accuracy and Billing Dos and Don’ts
November 05, 2021
Coding and billing accuracy is always a big challenge for urgent care. But since the beginning of the pandemic, we’ve seen a multitude of updates that seem to change without warning. In this issue of 3 Things to Know About RCM, you’ll learn how to improve E/M coding and billing accuracy with rigorous auditing by experts that have stayed abreast of the changes. You’ll also get the latest COVID-19 guidance from the Center for Disease Control (CDC) and Health and Human Services (HHS).
Wondering what flu season will look like? Whether it’s mild or severe, be sure you’re up to speed to administer vaccinations with our tips and handy clip-and-save chart.
Claims auditing is critical to solid documentation and E/M coding accuracy. But your coders and auditors’ interpretation of medical necessity may diverge from that of your clinical staff. How do you make sure everyone is on the same page? Use these three tips:
Audits force practices to neutralize subjectivity surrounding a particular patient or interaction and shift focus only to the hard facts.
For example: If a patient comes in with a request for a mole check and your office performs bloodwork, you’ll need to clearly demonstrate, via documentation, why the diagnostic testing is necessary. Or maybe you have an established patient coming in and the physician refills their prescription and talks about some minor lifestyle changes—such as the number of miles a patient runs per week—and your office is billing a level of E/M service that may be technically okay but isn’t ethically appropriate.
In scenarios like this, a formal internal audit looking at levels of service reported and medical necessity may bring up valid questions. If the documentation does not clearly demonstrate the medical necessity for the level of service billed, auditors must question the E/M level to ensure claim accuracy.
During your audit process look at the entire document – not just snippets. The Centers for Medicare & Medicaid Services (CMS) is looking at everything that’s included on that date of service. You should, too.
Find out how a physician ordering tests unsupported by a patient’s clinical record may be a problem in your practice by conducting internal and external audits. Audits give you an opportunity to identify red flags and adjust with specific providers to ensure your claims pass the documentation test. Be sure you can support the level of service and the whole record.
Telehealth has very specific rules of coverage. And like other visits, you can’t bill anything not medically indicated (and documented). The public health emergency (PHE) has loosened some of the restrictions on telehealth coding and billing, but the easing of rules really applies only to situations affected—at least tangentially—by COVID-19.
Cutting red tape surrounding telehealth would mostly affect services that were covered if a patient (who doesn’t have to have COVID or be tested for COVID) were to come into the office. This also applies to nonphysician providers (NPPs) whose telehealth services can be reimbursed under certain PHE-specific rules.
Important: Make sure you know and are following the guidelines as specified by CMS. Regulatory agencies are looking out for pandemic-related fraud and are now stepping up enforcement
Source: Medicare Compliance & Reimbursement – 2021; Volume 47, Number 20
Part of the confusion surrounding 99211 (Office or other outpatient visit for the evaluation and management of an established patient, that may not require the presence of a physician or other qualified health care professional. Usually, the presenting problem(s) are minimal) lies in the fact that, unlike all the other office and outpatient evaluation and management (E/M) codes, 99211 has no medical decision making (MDM) level requirements.
The confusion over the code may also increase after Jan. 1, 2022, when the words “usually, the presenting problem(s) are minimal” will no longer be a part of the code descriptor for 99211, suggesting the patient need not have any presenting problems in order for you to bill 99211. In fact, even after the change, you will still not be able to use the code to document a service that does not have an E/M component or use 99211 if the only service provided at the encounter is a service that has its own CPT® code.
When not to bill 99211
Services performed on their own, and that have their own CPT® code (such as routine venipuncture and immunizations or other injections) cannot be billed using 99211. Additionally, routine services such as blood pressure checks or prescription refills (providing no change in medication or dosage occurs) cannot be billed using 99211. Remember: If performed along with a separate and significant E/M service, including 99211, any service that can be documented with a CPT® code can be billed as well providing modifiers 25 (Significant, separately identifiable evaluation and management service by the same physician or other qualified health care professional on the same day of the procedure or other service) or 57 (Decision for surgery) are appended to the E/M, depending on encounter specifics.
When to bill 99211
If you have an order from your physician that the patient must be evaluated and that the service is medically necessary to manage a specific patient condition, or chief complaint, then you can justify billing 99211.
Source: Published in E/M Coding Alert – 2021; Volume 9, Number 10
Interested in more urgent care tips, best practices, and industry updates? Check out our August and September installments.
CTA: Interested in more? Our RCM experts use smart solutions and best practices to stay on top of revenue cycles and reimbursement. Learn how.
Flu vaccination season is in full swing, and the Centers for Disease Control and Prevention (CDC) has predicted “an early and possibly severe flu season” thanks to “reduced population immunity due to lack of flu virus activity since March 2020”.
So, whether your practice administers vaccines to a handful of your patients or operates a full-blown flu vaccination clinic, you need to update your knowledge of flu vaccination guidelines and recommendations now.
Here’s everything you need to know to get through the next few months.
First, know what hasn’t changed
On Aug. 27, 2021, the CDC’s Advisory Committee on Immunization Practices (ACIP) published its updated recommendations for, and continued guidance on, flu vaccinations.
The good news is that not a whole lot has changed for coding influenza vaccines and/or administration. The ACIP is still recommending “routine annual influenza vaccinations for all persons aged six months or older who do not have contraindications.”
Additionally, per the report, “ACIP makes no preferential recommendation for a specific influenza vaccine when more than one licensed, recommended, and age-appropriate vaccine is available.” So, providers can continue to use whichever quadrivalent flu vaccine they ordered earlier this year.
But the ACIP has provided the following updates.
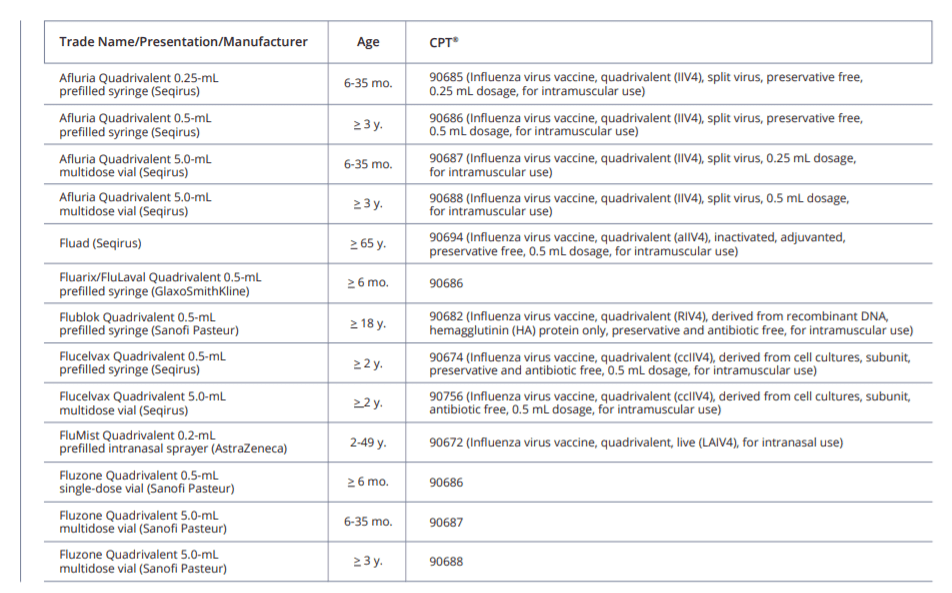
Beginning now, you can start to retire CPT® codes 90654, 90655-90660, 90661, and 90673 (Influenza virus vaccine, trivalent …). That’s because the ACIP report announced that “all seasonal influenza vaccines expected to be available for the 2021–22 season are quadrivalent.”
So, for this season, you’ll choose from the quadrivalent vaccines listed in the clip-and-save table at the end of this article.
Note: Two other CPT® quadrivalent codes—90630 (Influenza virus vaccine, quadrivalent (IIV4), split virus, preservative free, for intradermal use) and 90688 (Influenza virus vaccine, quadrivalent (IIV4), split virus, 0.5 mL dosage, for intramuscular use)—will not be in play for the 2021-2022 flu season.
As they have done in previous years, the CDC has changed the composition of the available quadrivalent vaccines, updating the influenza A(H1N1)pdm09 and influenza A(H3N2) components.
Both 90674 and 90756 are now appropriate for children 2 years of age and younger. This change occurred in March of 2021; prior to that, the vaccine was only approved for children 4 through under 18 years of age.
The ACIP sees no reason why your provider cannot co-administer an influenza vaccine with a COVID-19 vaccine at this time. However, the committee does recommend that your provider “should consult current COVID-19 vaccine recommendations and guidance for up-to-date information.”
This vaccination season, the ACIP has given the green light to vaccinating women in their third trimester “soon after [the] vaccine becomes available.” Children six months through two years needing two doses four weeks apart should also get their first dose “as soon as possible after [the] vaccine becomes available.” And nonpregnant adults should not get vaccinated early (before September) “unless there is concern that later vaccination might not be possible.”
The ACIP is also recommending that patients who have experienced a severe allergic reaction or anaphylaxis to various egg-based vaccines in the past should now receive their vaccinations “in an inpatient or outpatient medical setting under supervision of a provider who can recognize and manage a severe allergic reaction.” The ACIP is also now recommending providers consider consulting with an allergist to help identify the vaccine component responsible for the reaction.
And Don’t Forget the Following
Clip-and-Save Reference Table
In an effort to curtail the Delta variant and reduce COVID spread, the feds introduced a new comprehensive vaccination plan—and healthcare workers are among those impacted by the mandates.
Background: In August, the Centers for Medicare & Medicaid Services (CMS) issued a staff vaccination requirement for more than 15,000 Medicare and Medicaid-participating nursing homes, citing statistics that showed higher staff vaccination rates correlate to fewer residents contracting the virus. Then the Department of Health and Human Services (HHS) mandated vaccinations for all HHS healthcare workers and auxiliary agencies’ health workforce. In addition to the federal policies, several governors have also implemented COVID vaccination and weekly testing requirements for healthcare workers in their state
Now: On Sept. 9, the White House announced another round of COVID-19 vaccination mandate in its “Path Out of the Pandemic” action plan. “The Biden-Harris Administration will require COVID-19 vaccination of staff within all Medicare and Medicaid-certified facilities to protect both them and patients from the virus and its more contagious Delta variant,” CMS says in the release. “Facilities across the country should make efforts now to get health care staff vaccinated to make sure they are in compliance when the rule takes effect.”
Under this latest decree, CMS is expanding its emergency regulations to include “hospitals, dialysis facilities, ambulatory surgical settings, and home health agencies, among others,” and making the vaccination requirement “a condition for participating in the Medicare and Medicaid programs,” an agency release says.
“As the Delta variant continues to spread, we know the best defense against it lies with the COVID-19 vaccine,” says CMS Administrator Chiquita Brooks-LaSure in a release. “Data show that the higher the level of vaccination rates among providers and staff, the lower the infection rate is among patients who are dependent upon them for care.”
Important: Though only Medicare and Medicaid providers who receive federal funding must comply with the new healthcare provider mandates according to the latest guidance, there’s another prong to consider in the Biden plan.
“The Department of Labor’s Occupational Safety and Health Administration (OSHA) is developing a rule that will require all employers with 100 or more employees to ensure their workforce is fully vaccinated or require any workers who remain unvaccinated to produce a negative test result on at least a weekly basis before coming to work,” Biden’s plan says.
“OSHA will issue an Emergency Temporary Standard (ETS) to implement this requirement. This requirement will impact over 80 million workers in private sector businesses with 100+ employees.”
At press time, the feds hadn’t released an interim final rule on the implementation of the plan, timeline, costs, or the Medicare and Medicaid CoP tie-ins, nor had OSHA announced its part of the vaccination mandate rollout.
OCR Offers HIPAA Privacy Rule Guidance on COVID Vaccinations and the Workplace
With federal COVID-19 vaccination mandates for healthcare workers in the works, you might be confused about how that impacts HIPAA at your organization. The HHS Office for Civil Rights (OCR) appreciates the pressure on workers and employers to deal with these quandaries. To better help the public “navigate the COVID-19 pandemic,” the agency updated its online guidance on Sept. 30 with a fresh question-and-answer set on the who, what, when, and where of HIPAA and COVID-19 vaccines.
“We are issuing this guidance to help consumers, businesses, and healthcare entities understand when HIPAA applies to disclosures about COVID-19 vaccination status and to ensure that they have the information they need to make informed decisions about protecting themselves and others from COVID-19,” explains new OCR Director Lisa Pino in a release.
First, OCR reminds that the HIPAA Privacy Rule doesn’t affect all organizations or staff records, but rather “only applies to HIPAA covered entities (health plans, healthcare clearinghouses, and healthcare providers that conduct standard electronic transactions), and, in some cases, to their business associates,” the agency emphasizes.
Breakdown: Though there are only five HIPAA Q&As offered in the new COVID guidance, OCR provides covered entities (CEs) and their business partners (BAs) with a wealth of handy tips and examples for dealing with privacy concerns surrounding employee vaccinations.
The first question focuses on whether the Privacy Rule comes into play when CEs or BAs ask their staff if they’ve received the COVID-19 vaccination. According to OCR, it doesn’t. The Privacy Rule neither regulates nor prohibits CEs and BAs from “request[ing] information from patients or visitors,” including asking about COVID-19 vaccinations, OCR maintains in Answer No. 1. However, CEs and BAs should note that the Privacy Rule “does regulate how and when a covered entity or its business associate may use or disclose information about an individual’s vaccination status,” the agency cautions.
Tip: For example, OCR refers to this common scenario: a home health agency asks its employees if they’ve gotten the COVID vaccination. In this case, the Privacy Rule does not apply because the HHA is merely asking, not using, or disclosing the information, the guidance says.
The other Q&As touch on these concerns and whether the Privacy Rule applies individuals’ disclosure of their personal PHI to others; vaccination mandates and employment terms and conditions; workforce vaccination records and how to document, store, and keep them confidential; HIPAA authorizations; mask requirements; patient/public requests for healthcare workers’ vaccination status; and permitted disclosures of COVID-19 vaccination status for public health emergency (PHE) reasons.
Resources:
Source: Health Information Compliance Alert – 2021; Volume 21, Number 10
Interested in more urgent care tips, best practices, and industry updates? Check out our September and October installments.
Interested in more? Our RCM experts use smart solutions and best practices to stay on top of revenue cycles and reimbursement.
Join over 20,000 healthcare professionals who receive our monthly newsletter.

Join over 20,000 healthcare professionals who receive our monthly newsletter.