At a time when technology is embedded in our daily lives, it may be surprising that some doctors still use paper health records. Meaningful Use incentivized many to transition from paper records to EMRs (Electronic Medical Record systems) and EHRs (Electronic Health Record systems.) But according to the most recent available data from the CDC/National Center for Health Statistics, over 14 percent of office-based physicians still use paper.
These holdouts give various reasons for not using electronic systems for health and medical records. From cost, to implementation, to learning curves. However, without this transition, complete interoperability is not possible.
Read how an urgent care center switched from paper records to an EMR >>
In healthcare, interoperability gives providers access to all medical data for their patients. Most importantly, the data, security, and accuracy of interoperability improve patient outcomes.
Although the terms EMR and EHR are often used interchangeably, there are technically significant differences. We’ll define the differences between the two systems, explain when each should be used, and cover some of the most relevant benefits to providers, patients, and healthcare in general.
[cta_content id=”19237″]
What is an EMR (Electronic Medical Records System)?
An electronic medical records system is a digital version of a single patient’s medical chart. The EMR is primarily used by providers for diagnosis and treatment. It includes:
- Medical history
- Immunization dates
- List of allergies
- Visit record
- Diagnosis
- Treatment plan
Specific medical data is at the heart of an electronic medical records system. An effective urgent care EMR streamlines the charting process by learning provider preferences over time and making smart suggestions about diagnosis and treatment based on historical data. The EMR stores patient data over time, allowing providers quick access to important information that may affect treatment. It also serves as a legal record of an office visit.
An EMR effectively eliminates paper charts. Although EMR use is generally restricted to intra-office communication, it can be shared with other clinics, labs, or service providers.
Learn 10 ways to improve staff transition to a new EMR >>
What is an EHR (Electronic Health Records System)?
If an EMR is a snapshot of a patient’s medical history, the EHR is the whole movie. While EMRs focus on an urgent care visit or treatment path, EHRs encompass clinical data about a patient’s long-term healthcare and wellbeing.
EHRs rely on EMRs. Healthcare providers aggregate much of the data stored in EHRs from medical records created during patient encounters. A patient’s EHR is built over time, pulling in medical information from EMRs and other sources, including:
- Past medical history
- Demographic information
- Immunization dates
- Blood type
- List of allergies
- Lab results
- Radiology images
- Progress notes
- Encounter notes
- Physician recommendations
- Diagnoses
- Medication history
- Past procedures
- Data imported from personal wellness devices
EHR medical histories stay with a patient throughout their life. They are accessed by various physicians, specialist healthcare professionals, and services like pharmacies and laboratories. A patient’s EHR ensures their healthcare providers have up-to-date information about allergies, medications, past illnesses, and treatment plans.
Electronic health records systems prioritize interoperability so professionals in different specialties and organizations can access a patient’s EHR data. They use standard data formats and are designed to share information securely with authorized healthcare professionals.
This feature film of a patient’s medical record is fluid, repeatedly updated with each healthcare touchpoint. With the constant changes and the inclusion of more and more records, the benefits of EHRs will increase for both patients and practitioners.
Make EHR selection easier with these 50 questions >>
The History of Electronic Health Records
Electronic health records systems first appeared in the 1960s. Hospitals like the Mayo Clinic struggled to cope with the enormous volume of paper records. A rudimentary EMR system allowed them to reduce record management cost and complexity.
Over time, the types of data stored in EMRs expanded, and they eventually became what we would today would call an EHR. At the time, the technology to support EHRs was expensive, so only large hospitals could afford to digitize. But doctors soon found digitized medical data had benefits beyond paper reduction.
EHRs offer a complete record of a patient’s medical history and treatment. This detailed overview improved diagnostic accuracy and ensured consistent treatment. It also enhanced communication and information sharing between doctors and specialists.
As technology evolved throughout the 1970s and 1980s, EHRs were adopted by most large healthcare providers. By the late 1980s and into the 1990s, reduced computer costs allowed smaller organizations like urgent care facilities to replace paper-based records with more focused electronic medical records systems.
The U.S. Government recognized the healthcare potential of EHR systems. In the early 2000s, it created the Office of the National Coordinator for Health Information Technology, kicking off a program to give all Americans electronic healthcare records within 10 years.
EHR Security: How Safe are Electronic Health Record Systems?
Patients must have confidence in their healthcare provider’s EHR or EMR system. They need to trust their private healthcare data is protected. In the U.S., EHR security and privacy are governed by HIPAA, the Health Insurance Portability and Accountability Act.
HIPAA’s Privacy Rule and Security Rule require protections for electronic private healthcare information (ePHI). EHR security measures include:
- Access controls so only authorized people can see electronic health records.
- The encryption of stored information so it can’t be read without a decryption key.
- An audit trail to record who has seen private healthcare data.
- If healthcare data does leak from EHR or EMR systems, healthcare organizations are legally required to notify users.
What is Certified Electronic Health Records Technology (CEHRT)?
CEHRT is a certification for electronic health record systems developed by the Office of the National Coordinator for Health Information Technology. It evaluates EHR system interoperability, secure information storage and exchange, and meaningful use. Healthcare providers who want to participate in federal incentive programs like the Medicare and Medicaid EHR Incentive Programs must use CEHRT EHR systems.
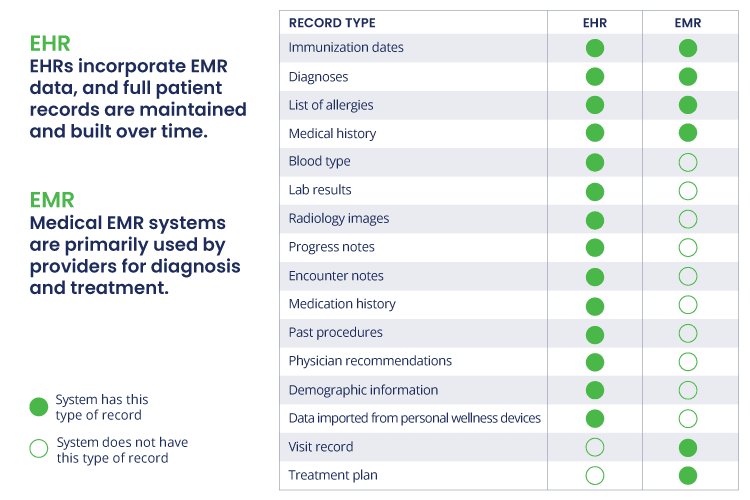
What is the Difference Between an EMR and EHR?
If you’re skimming for quick answers and just want a high-level overview of the difference between an EMR system and HER software, this table might help.
When to use an EHR vs EMR: is Patient Information the Only Consideration?
EHRs are robust solutions that provide the kind of information well-suited for larger systems like hospitals. We speak to the EHR a lot here because these healthcare giants represent a significant percentage of potential software users. However, there is a very specific instance when EMRs are superior to EHRs: urgent care.
Episodic care is very different from other types of patient care, and one of the biggest disadvantages of an EHR is it doesn’t support the efficiency that is vital to on-demand healthcare. An urgent care EMR and practice management (PM) system — especially one that is purpose-built for urgent care — provides a workflow that makes sense for these users. Customized templates exclude extraneous fields and other workflow bottlenecks that slow down the patient journey.
In an Experity case study, Dr. James Yost of CRH Healthcare reported that charting with the Experity EMR allows him to complete charting in about 45 seconds compared to the four or five minutes it used to take.
The more patients and urgent care can see in a day, the more revenue potential they have. That means the goal for many of these clinics is to have a door-to-door time of about 45 minutes. And that can be extremely challenging when using an EHR in an on-demand setting.
Learn more about EMRs in How to Choose the Best EMR for Urgent Care
How EMRs/EHRs Affect the Future of Healthcare
Technology is no longer something separate from our everyday lives, but instead, something that is as ubiquitous as the air we breathe. There is perhaps no better use of technology than improving the way we deliver medical care. If we are to see the transformations that are possible across every sector of the healthcare industry, we must face a few challenges and find solutions.
Interoperability is one of the biggest bridges yet to cross. From doctor to patient and lab to hospital, technology must improve the way our devices and systems communicate. EHRs must be designed to work together for the good of the community. Interoperability standards and the implementation of best practices and standards will continue to guide healthcare and medical technology toward this overarching goal.
The fine line between EMRs and EHRs is ambiguous — many EMRs record some of the same information as EHRs. Others are specifically an electronic chart. Advancing technology and increased participation by patients and providers will continue to change the way healthcare is delivered and foster even more innovation.
As medical records become increasingly digitized, the development of a comprehensive, secure health information exchange (HIE) will provide the healthcare community data needed to identify trends, trace the efficacy of new treatments and medications, share successes, collaborate, and improve healthcare for all.
Want to learn more about how an EMR will transform your urgent care?